How to Audit Medical Cabinet Access and Storage Compliance in a Care Home
March 25, 2026

Medical cabinet compliance is not something that can be checked once and forgotten. In a care home, medicines storage is a live system. Staff change. residents’ needs change. medicine rounds evolve. cabinet access routines can drift over time. A cupboard that was secure and well managed six months ago may now have weak key control, unclear ownership or poor record alignment. That is why regular auditing matters.
A medicines storage audit helps a care home check whether cabinet access, cupboard security, key control and day-to-day practice still match the provider’s policy and the needs of the people receiving support. It also helps identify whether the written system and the real system are still the same thing. In many homes, that is where the most useful findings come from.
This guide explains how to audit medical cabinet access and storage compliance in a care home, what points to review, what evidence to check and how to turn findings into practical improvements. For the wider storage picture, see our comprehensive guide to medical cabinets. You may also want to read Medical Cabinet Key Management in Care Homes, How to Carry Out a Medicines Storage Risk Assessment in a Care Home and Best Lock Types for Medical Cabinets in Care Homes and Clinics.
Why a Medicines Storage Audit Matters
Secure storage is only part of good medicines management. A care home also needs clear access control, practical procedures, accurate records and a system that staff can follow consistently. Auditing helps confirm that these elements are working together.
Without regular audit, problems can build up quietly. A cabinet may still lock properly, but too many people may have keys. A keypad code may not have been changed after staffing changes. A room-based cupboard for self-administration may no longer reflect the resident’s current ability. A key register may exist on paper but no longer match what staff are actually doing. None of these issues always causes an immediate incident, but each one weakens the overall system.
The purpose of audit is not to create blame. It is to check whether the storage model still works, whether risks are controlled and whether the home can show that medicines access is secure, proportionate and properly governed.
What a Storage Compliance Audit Should Cover
A strong audit looks beyond the cabinet itself. It should cover the storage environment, the access method, the records behind the system and the way staff use it in practice. Focusing only on whether the cupboard door locks misses most of the real risk.
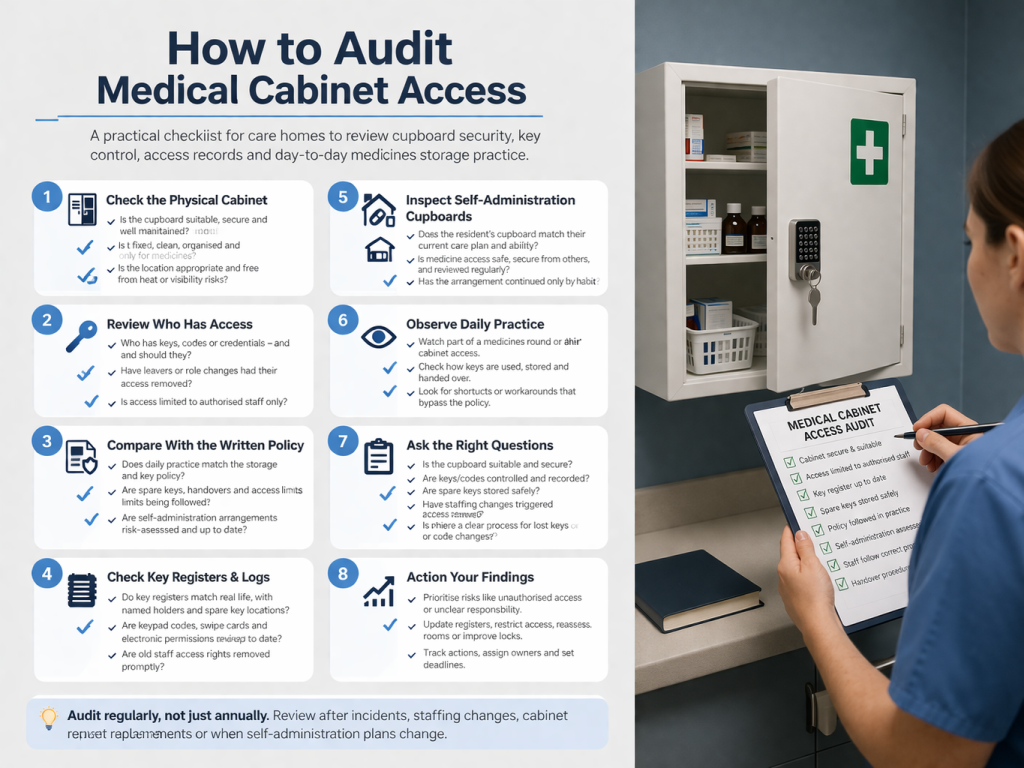
In most care homes, a practical audit should review five main areas:
- the physical cabinet or cupboard
- the access control method
- the people who use the system
- the supporting records and policy documents
- the actual day-to-day workflow around storage and access
Looking at all five gives a much clearer picture than a basic visual inspection.
Start With the Physical Storage
The first part of the audit is the cabinet or cupboard itself. Is the storage unit still suitable for the medicines being held? Is it in good condition? Does the lock work properly? Is the cabinet fixed and positioned appropriately? Is it clean, organised and used only for its intended purpose?
In central medicines areas, the audit should also consider whether the cupboard remains suitable for current stock levels and whether medicines are segregated in a way that reduces selection error. In residents’ rooms, the audit should check whether the cupboard still matches the care plan and whether the location allows safe but controlled access.
It is also worth checking the surrounding environment. A medicines cupboard may be technically sound but badly located. For example, a cabinet near a heat source, a cupboard placed where others can observe or access it too easily, or a room layout that makes safe staff access awkward during busy rounds can all weaken the wider system.
Audit Who Has Access
Once the physical storage has been reviewed, the next question is access. Who can open the cupboard? How many people have keys, codes or electronic credentials? Is that number still appropriate? Does access reflect current roles rather than historic arrangements?
This is one of the most important parts of the audit because cabinet compliance often fails through over-broad access. A secure cupboard is far less secure if nobody can say clearly who is authorised to open it. The home should be able to show that access is restricted to the right people and that any wider access has a clear reason.
In practice, that means checking issued keys, keypad codes, swipe cards, electronic key permissions and any master access arrangements. It also means checking whether the current access list still matches the actual staff team. If a member of staff has left, changed role or no longer needs access, the system should show that this has been dealt with properly.
Compare the Real System With the Written Policy
An audit should always compare live practice with the written policy. Many care homes do have medicines policies and key-management procedures, but the most useful question is whether staff are following them in day-to-day work.
For example, the policy may say spare keys are stored securely, but is that happening in practice? The policy may say access is restricted to authorised staff, but do agency staff receive access informally? The policy may say key handover is recorded, but can staff actually show consistent evidence of this? The policy may refer to risk-assessed self-administration, but do the room-based cupboard arrangements still reflect current resident reviews?
This comparison matters because compliance is about the operating system, not just the document set. A policy that looks strong but is not used properly will not withstand scrutiny and, more importantly, will not protect residents as intended.
Review Key Registers and Access Records
If the home uses physical keys, the key register should be part of every audit. Check how many keys exist for each cupboard or lock suite, who each one is issued to, which keys are held as spares and whether master keys are recorded separately. The register should be current, not historical.
Look for warning signs such as incomplete entries, keys with no named holder, spare keys with no secure location recorded, or register entries that do not match what staff report during the audit. These are often the early indicators that the system has become informal.
If the home uses electronic access, review the equivalent information. Who holds active access rights? When were they last reviewed? Are there audit logs available? Are old credentials removed promptly when staff leave or change role? A digital system can be excellent, but only if someone actually manages it.
In homes where access logs or audit trails exist, use them. They can help confirm whether the cabinet is being opened by the right people, whether access patterns look sensible and whether temporary workarounds have become embedded in the routine.
Check Self-Administration Arrangements Separately
Self-administration cupboards should not be audited in exactly the same way as staff-only medicines cupboards. The purpose is different. In these cases, the audit should confirm that the resident’s storage arrangement still matches the current risk assessment and care plan, and that medicines remain secure from other people while still being accessible to the resident when needed.
Check whether the resident still manages the cupboard safely, whether support arrangements are clear, whether the cupboard remains suitable for the medicines being stored and whether other people could gain access. In shared or busier settings, this point matters a great deal. A room-based cupboard may be acceptable in principle but no longer suitable if circumstances around the resident or room have changed.
It is also worth checking whether room-based arrangements are being reviewed as part of normal care planning or whether they have simply continued by habit.
Observe Practice, Not Just Paperwork
One of the best ways to improve a storage audit is to include direct observation of how the system works. Paperwork can tell you what should happen. Observation shows what does happen.
That might include watching part of a medicines round, observing how staff access a central cupboard, checking whether keys are kept secure during use, or seeing how a shift handover handles cupboard access responsibility. You are not looking to catch people out. You are trying to understand whether the process is practical and stable.
Observation often reveals issues that records do not. For example, a key may officially be signed to one person but be passed around informally during the round. A cupboard may officially be locked when not in use but stand open for convenience during busy periods. A keypad code may officially be controlled but be known by too many people. These findings are extremely useful because they show where the real process differs from the intended one.
Questions to Ask During the Audit
A good audit is built around clear questions. The exact format can vary, but the following points usually give a strong framework:
- Is each medicines cupboard or cabinet suitable for its current purpose?
- Is the cupboard clean, secure, well maintained and properly organised?
- Who currently has access, and is that still appropriate?
- Are keys, codes or credentials controlled and recorded?
- Are spare keys stored securely?
- Does the key register or access log match current practice?
- Are self-administration cupboards aligned with current risk assessments?
- Are staff following the written procedure in daily work?
- Have access rights been reviewed after staffing changes?
- Is there a clear process for lost keys, code changes or emergency access?
- Are there any workarounds in use that weaken the storage system?
- Have previous audit findings been acted on?
These questions move the audit beyond a basic pass-or-fail inspection and turn it into a useful operational review.
Common Findings That Audits Often Reveal
Many audit findings are not dramatic. They are usually small weaknesses that have built up over time. Common examples include duplicate keys with no clear record, spare keys kept in the wrong place, master keys issued more widely than necessary, old keypad codes still in use after staffing changes, room-based cupboards that have not been reviewed recently, and medicines cupboards that are secure in theory but poorly organised in practice.
Another common finding is that policies are broadly correct but too generic. Staff may understand the principle of secure access but not the exact local process for this site, this cupboard layout and this staffing model. Where that happens, the provider may need to tighten the operational detail rather than rewrite the whole policy from scratch.
Audits also often reveal that the service has outgrown the original access method. A simple key system that worked in a smaller home may become harder to manage once staffing numbers increase, agency use rises or several cupboards need to be accessed across different parts of the building.
Turning Findings Into an Action Plan
An audit should end with more than a checklist. It should produce a clear action plan. Each finding should lead to a decision about what needs to change, who is responsible and when the change will be completed.
For example, the action may be to update the key register, restrict master-key access, change keypad codes, re-assess a resident’s self-administration cupboard, replace a worn cabinet lock, or rewrite the handover process so cupboard responsibility is recorded more clearly. In some homes, the action may be more structural, such as moving from a loose physical key system to a more controlled electronic access model.
Prioritisation matters. Findings that affect unauthorised access, unclear responsibility or current medicines security should be dealt with first. Lower-level housekeeping issues can follow, but they should still be tracked so they do not remain open indefinitely.
How Often Should You Audit?
The right frequency depends on the size of the home, the complexity of its medicines processes and whether there have been recent changes or incidents. Many homes benefit from combining routine scheduled audits with additional targeted reviews after trigger events.
- regular planned audits as part of medicines governance
- extra review after an incident or near miss
- review after major staffing changes
- review after cabinet replacement, lock changes or refurbishment
- review when self-administration arrangements change
- review when a new access method, such as keypad or card access, is introduced
The key point is consistency. A short, regular audit process usually works better than a long audit that happens too rarely.
Who Should Carry Out the Audit?
The audit should be led by someone who understands medicines governance and the local storage system. Depending on the home, that may be the manager, deputy manager, clinical lead, medicines lead or another authorised senior member of staff. What matters is that the auditor understands both the written process and the operational reality.
Some providers also find it useful to include a second perspective, especially if the storage system has become routine and familiar. A fresh pair of eyes can spot drift that local teams have stopped noticing. The audit still needs local ownership, but it can benefit from challenge.
Where specialist products or more advanced electronic locking systems are in use, the provider may also need technical input on maintenance, permissions or system reports. The audit should stay practical, but it should be technically informed where needed.
How to Use Audit Results to Improve Procurement Decisions
Audit findings are useful for more than compliance. They can also guide better purchasing decisions. For example, if repeated audits show weak control over shared keys, the home may need to consider a different lock format or a better-managed access method. If cupboards are consistently overcrowded or poorly organised, the issue may be cabinet size or layout rather than staff performance.
This is why storage compliance and cabinet specification should not be treated as separate conversations. Audits often reveal whether the product choice still fits the care model. A cupboard that suited the service three years ago may not be the best fit now. The stronger the audit process, the easier it becomes to buy on evidence rather than assumption.
Common Audit Mistakes to Avoid
It is easy for a medicines storage audit to become too narrow. Some common mistakes reduce its value:
- checking only the cupboard condition and ignoring access control
- reviewing paperwork without observing real practice
- auditing staff-only cupboards but forgetting self-administration storage
- accepting a policy at face value without checking local use
- failing to follow up previous findings
- treating key control as a minor issue instead of part of medicines governance
- not checking whether staffing changes have altered access risk
The best audits are balanced. They look at the cabinet, the access method, the records and the daily routine together.
Final Thoughts
Auditing medical cabinet access and storage compliance is one of the simplest ways to keep a care home’s medicines system strong over time. It helps confirm that cupboards are secure, access is controlled, records are accurate and real practice still matches the written process. Just as importantly, it helps the home spot drift before that drift becomes an incident.
A useful audit is not just a cupboard inspection. It is a review of the whole access system: the cabinet, the lock, the key or credential, the staff routine, the resident’s needs and the documents that tie it all together. When that review happens regularly and leads to action, medicines storage becomes easier to manage and easier to trust.
If you are reviewing storage across your site, explore our Medical Cabinet Security range and return to our comprehensive guide to medical cabinets for broader planning guidance across healthcare and care environments.
Discover more from Blog Total Locker Service
Subscribe to get the latest posts sent to your email.