Controlled Drugs in Care Homes: Storage, Record Keeping and Key Control
March 26, 2026
Controlled drugs need a higher level of control than most other medicines. In a care home, that means more than simply locking a cupboard. Staff need a clear system for storage, access, recording, stock checks, discrepancies and disposal. When those processes are weak, the risk is not only theft or diversion. It is also missed doses, inaccurate balances, poor handovers and avoidable harm to residents.

For care homes, the safest approach is to treat controlled drugs as part of a wider medicines governance system. Storage, cabinet choice, key control, MAR records, the controlled drugs register and disposal arrangements all need to align. That is especially important where several staff members administer medicines across different shifts, or where residents move in and out of hospital with changing prescriptions.
This guide explains the practical points care homes should cover when managing controlled drugs day to day, with a particular focus on secure storage and audit-ready record keeping. It is written for providers reviewing their medicines room, cabinet layout and procedures as part of safer care home practice.
What controlled drugs are in the care home setting
Controlled drugs are medicines that are subject to additional legal controls because they may be misused, obtained illegally or cause harm. In the care home setting, providers need to comply with the Misuse of Drugs Act 1971 and the related regulations when storing, handling and recording these medicines.
In practice, care homes often see controlled drugs used for pain relief, palliative care, symptom control and some neurological or psychiatric needs. Examples can include morphine, diamorphine, methadone, fentanyl, oxycodone and ketamine.
Why controlled drugs need tighter control
The main risks are straightforward. These medicines can be clinically important, sometimes time-sensitive, and attractive for diversion or misuse. That means care homes need systems that protect residents while also making it easy to identify discrepancies quickly.
Good control also supports continuity of care. When records are current and stock is organised properly, staff can see what has been received, what has been given, what remains in stock and what is awaiting disposal. That reduces confusion during handovers, after hospital discharge or when a prescription changes.
Which controlled drugs must go in the controlled drugs cupboard
This is one of the most important practical questions for care homes. Unless a person is looking after their own medicines, Schedule 2 controlled drugs should be stored in a controlled drugs cupboard and recorded in the controlled drugs register.
Certain Schedule 3 controlled drugs, including buprenorphine and temazepam, must also be stored in the controlled drugs cupboard, although Schedule 3 drugs do not need to be recorded in the controlled drugs register. Other Schedule 3 drugs, such as midazolam, pregabalin, gabapentin and tramadol, do not all have the same storage requirement. Schedules 4 and 5 do not need to be stored in the controlled drugs cupboard or recorded in the controlled drugs register, but they still need secure storage and accurate records of receipt, administration and disposal.
That distinction matters for cabinet planning. A care home needs enough secure storage to separate medicines properly, but the dedicated controlled drugs cupboard should not become a catch-all for every medicine simply because it is convenient.
What a compliant controlled drugs cupboard should support
A controlled drugs cupboard should meet the relevant safe custody requirements, and the supplier should be able to confirm whether a cupboard is compliant. It should not be used to store unrelated items such as jewellery or money, and access should be restricted according to need.
For care homes reviewing cabinet security, that has several practical implications. The cupboard needs to be fit for purpose, installed properly and clearly reserved for controlled drug storage. Spare keys should be stored securely, and the home should decide through risk assessment who is authorised to hold keys.
In day-to-day use, the cupboard also needs to support clean organisation. Different residents’ medicines should be identifiable, old stock should not sit mixed with current stock, and high-use items should not create clutter that makes stock checks harder. A secure cupboard is only part of the answer. The internal organisation matters just as much.
Key control and access management
Key control is one of the areas where weak practice can quietly undermine an otherwise good medicines system. If several people have casual access, if spare keys are poorly stored, or if there is no clear shift handover for keys, accountability becomes blurred very quickly.
For care homes, that usually means having a written process covering who may hold the keys, where spare keys are kept, what happens during shift change, and what staff should do if keys are missing or a discrepancy is found. A stronger policy also sets out who must be informed if an incident occurs.
The controlled drugs policy should be specific
Care homes should have a policy or standard operating procedure for controlled drugs. It should cover ordering, storing, administering, recording and disposal. That policy should not be vague. Staff need practical instructions that match the home’s real cabinet layout, key arrangements, MAR process and escalation route.
A good controlled drugs procedure should explain where stock is stored, who has access, how receipt is checked, how balances are updated, how administration is recorded, how returns and destruction are handled, and what happens if stock and records do not match. It should also cover transdermal patches and refrigerated items, because these can be missed if the procedure focuses only on tablets and liquids.
Record keeping: the register and the MAR both matter
Care homes sometimes focus heavily on the cupboard and not enough on the paperwork. In reality, record keeping is what proves control. Any movement of a Schedule 2 controlled drug should be recorded in a controlled drugs register. The register should be a bound book with numbered pages and used to record receipt, administration, disposal and transfer of controlled drugs held by the care home.
Alongside the controlled drugs register, the MAR still matters. Care home medicines administration records should include the person’s full name, date of birth, the medicine name, formulation, strength and dose, route, allergies or reactions, monitoring or review requirements where appropriate, and special instructions such as whether the medicine should be taken before, with or after food. Records should also be updated when medicines change.
The safest process is to make sure the register, the MAR and the physical stock tell the same story. If one says a dose was given, the others should support that. If stock balances drift away from the register, or if a resident returns from hospital with a changed medicine list, the records need to be reconciled before normal routine resumes.
Running balances and witnessed checks
Care homes should keep a running balance of the stock level of each controlled drug preparation. That is one of the simplest and strongest safeguards in routine practice. It means discrepancies are more likely to be found when they occur, rather than days or weeks later.
It is also good practice for two trained and competent members of staff to witness and sign when controlled drugs stock is received, when stock balances are checked, when controlled drugs are administered and when they are disposed of. Even where the law does not demand two signatures in every case, the practice is still a strong control measure in care homes because it reduces ambiguity and strengthens the audit trail.
Refrigerated controlled drugs
Some controlled drugs also need refrigeration. If a controlled drug has safe custody requirements and needs to be kept in a fridge, it should be stored in a locked medicines fridge. Standard medicines fridges do not meet the same safe custody rules as a controlled drugs cupboard, so the safest approach is often to keep the controlled drug in a lockable box within the locked fridge and restrict access. Other medicines may be stored in the same fridge, but separately.
That has a direct impact on medicines-room planning. Fridge layout, lockable internal boxes and restricted access all need to be considered as part of the storage system, not added later as an afterthought.
Self-administration and resident access
Not every controlled drug in a care home is centrally administered. People should be able to access medicines when needed, including controlled drugs, where self-administration is appropriate. Storage for self-administration should be identified in the person’s care plan, such as a lockable cupboard or drawer in the person’s room, and it must not be accessible to other people.
That means a care home may need more than one secure storage approach. A main controlled drugs cupboard may be right for centrally managed medicines, but an individual resident may need a separate lockable arrangement in their own room if they are assessed as suitable to self-administer. The key point is that access and risk are assessed deliberately, not assumed.
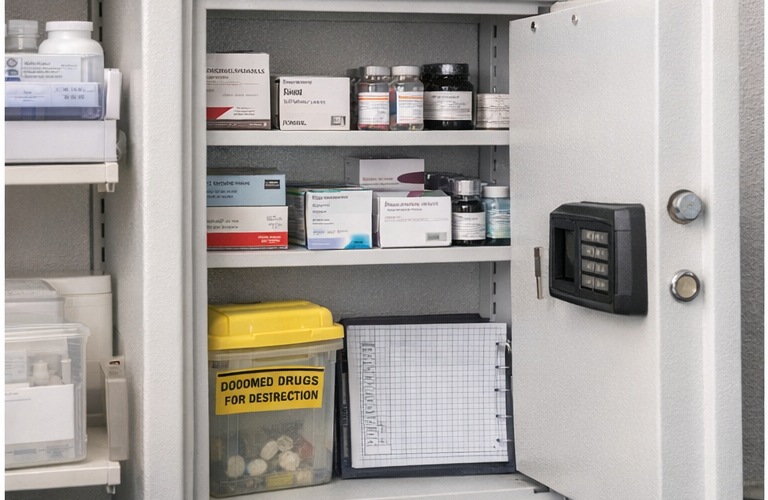
Disposal and out-of-date stock
Controlled drugs awaiting disposal should not remain mixed with current stock. Care homes should keep records of medicines, including controlled drugs, that have been disposed of or are waiting to be disposed of. Medicines awaiting disposal should be kept in a locked cupboard until they are collected or taken to the pharmacy.
In care homes without nursing, unwanted or out-of-date controlled drugs should be separated from current stock, stored in line with policy and returned promptly to a community pharmacy for destruction, with a record made in the controlled drugs register and witnessed by another suitably trained person. In care homes with nursing, requirements differ because some controlled drugs must be denatured before disposal, and destruction of Schedule 2 stock requires an authorised witness.
For providers, the practical lesson is simple: disposal needs its own process, its own storage step and its own records. Old medicines should not be left sitting in the active cupboard because nobody is sure what to do next.
Common weaknesses care homes should look for
The most common problems are usually procedural rather than dramatic. A cupboard may be compliant, but keys are handed around casually. The register may exist, but balances are not checked routinely. Stock may be secure, but discontinued items remain mixed with active medicines. Refrigerated controlled drugs may be locked, but not clearly separated. The policy may mention discrepancies, but staff are not confident about who to contact.
A useful review looks at the whole pathway: cabinet, keys, receipts, administration, register entries, MAR accuracy, stock checks, returns and destruction. That is usually where care homes discover whether the system is genuinely strong or only looks tidy on the surface.
Final thoughts
Controlled drugs management in care homes depends on more than a locked door. It requires a secure and suitable cupboard, clear key control, accurate register entries, up-to-date MAR records, routine balance checks and a disposal process that keeps old stock separate from current medicines.
For care homes reviewing their medicines room, this is also a storage-design issue. The right cabinet setup, internal organisation and access control can make safe practice much easier to maintain every day. When the storage system supports the workflow, staff can check stock faster, keep cleaner records and respond more confidently during audits, inspections and handovers.
If you are reviewing medicines storage for controlled drugs, choosing a suitable medical cabinet and creating a clear controlled drugs process can help support safer administration, better record keeping and stronger day-to-day governance.
“`
Discover more from Blog Total Locker Service
Subscribe to get the latest posts sent to your email.